


Point-of-care Ultrasound Diagnosis of Tennis Leg


The British Medical Ultrasound Society
24th Jul 2024
These sports injury examples have kindly been provided by our BMUS MSK Special Interest Group. A special thank you to Catharine Berry, consultant radiographer at Leicester University Hospitals, who is Chair of the group.
1. Ulnar collateral ligament (UCL) injuries of the Thumb
2. Knee tendinopathy through overuse
8. Long head of biceps (LHB) subluxation
9. Stress fractures: long distance runners
Traditionally referred to as ‘skier’s thumb’ ulnar collateral ligament injuries of the MCP joint can occur when there is forced hyperabduction of the thumb by a ski pole. This is also a common injury seen in rugby players when the ball is caught and the thumb is forcibly pulled back.
Injury can cause partial or complete rupture of the ulnar collateral ligament. It most commonly detaches from its insertion site at the proximal phalangeal base.
The UCL normally lies deep to the adductor pollicis longus tendon. If the UCL is ruptured the torn end can sometimes slip over the adductor aponeurosis preventing it from returning to its natural anatomical position, causing a bump known as a Stener lesion. Stener lesions require surgical intervention. Further reading:
Rupture of the ulnar collateral ligament of the thumb – a review - PMC (nih.gov)
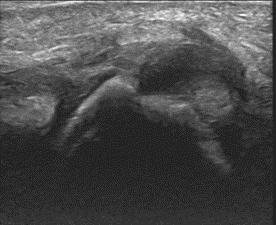
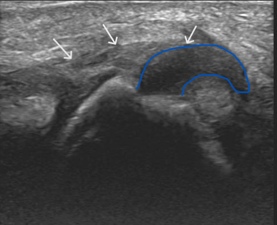
Long axis ultrasound of the thumb at the level of the metacarpophalangeal joint.
The white arrows demonstrate the adductor pollicis aponeurosis. The blue trace outlines the torn and retracted ULC from the base of the proximal phalanx. It has flipped proximally – lying superficial to the aponeurosis.
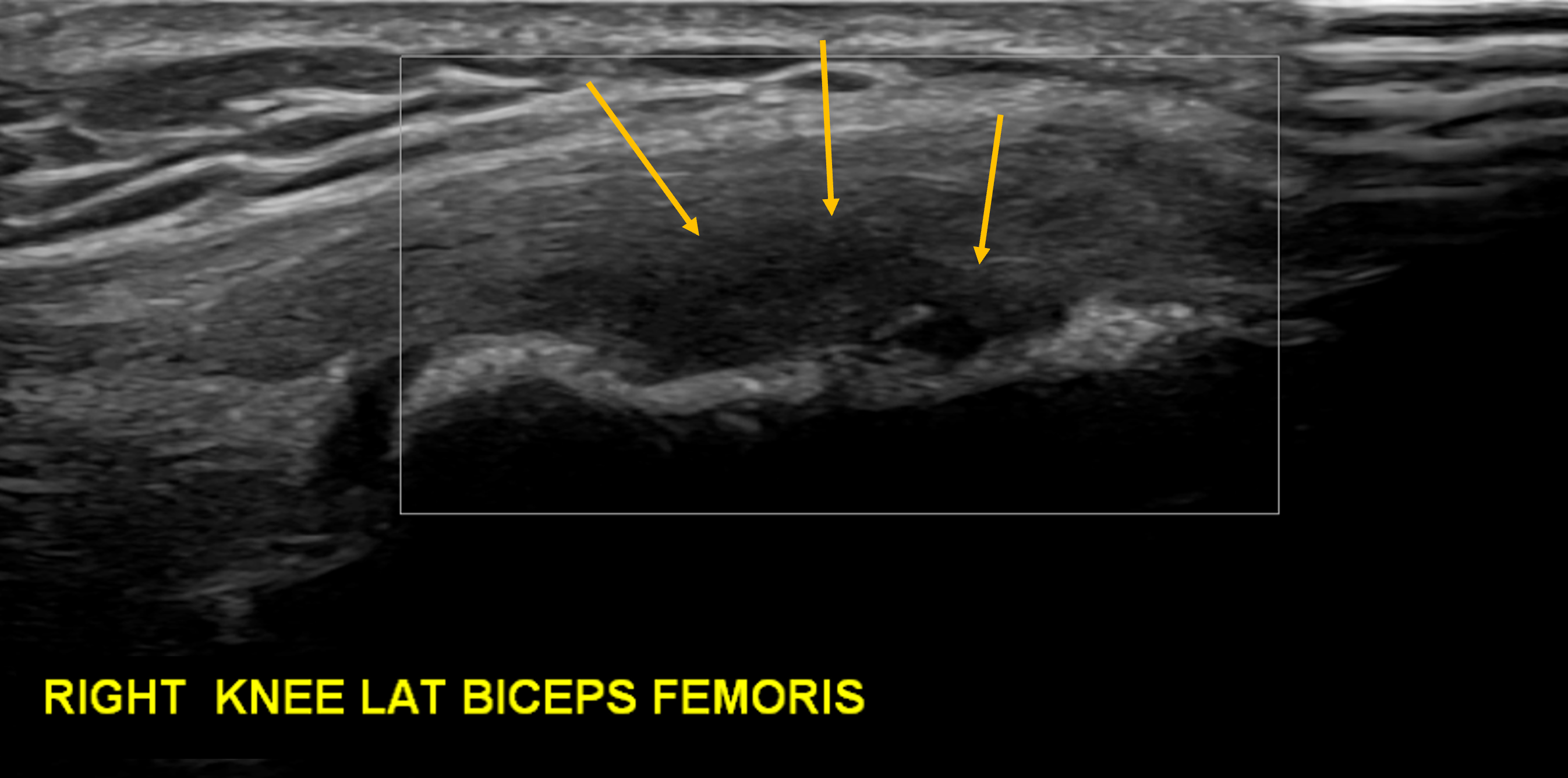
This is an overuse condition triggered by sports where there is repetitive acceleration and deceleration, such as running and football. This patient is a triathlete. The image demonstrates a loss of the normal fibrillar pattern at the BF insertion (arrows) in keeping with tendinopathy. There was no neo-vascularity present.
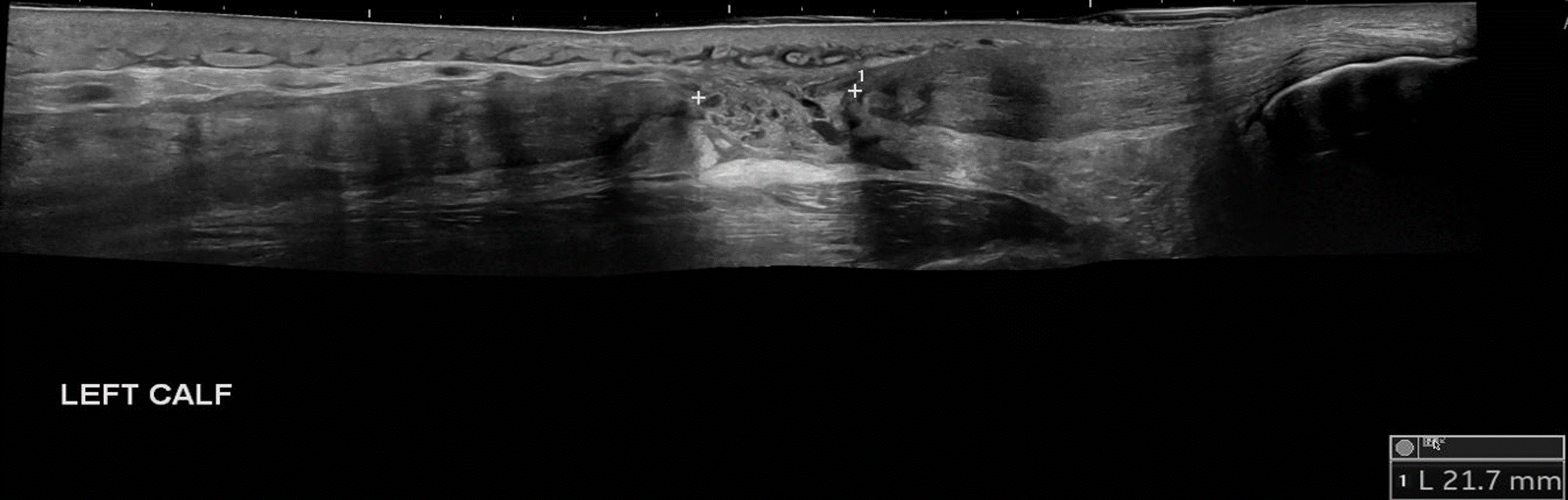
Athletes in running sports have a high incidence of Achilles tendon overuse injuries. About 75% of total tendon ruptures and the majority of partial tendon ruptures are related to sports activities usually involving abrupt repetitive jumping and sprinting movements.
The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. Ultrasound findings demonstrated here show a complete Achilles tendon rupture, the measurement is of the gap width between the tendon free edges. Oedema is noted filling the gap.
To find out more about Achilles tendon ruptures:
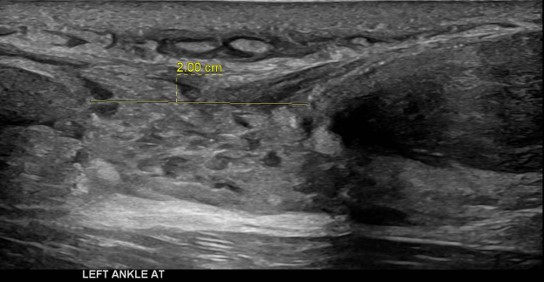
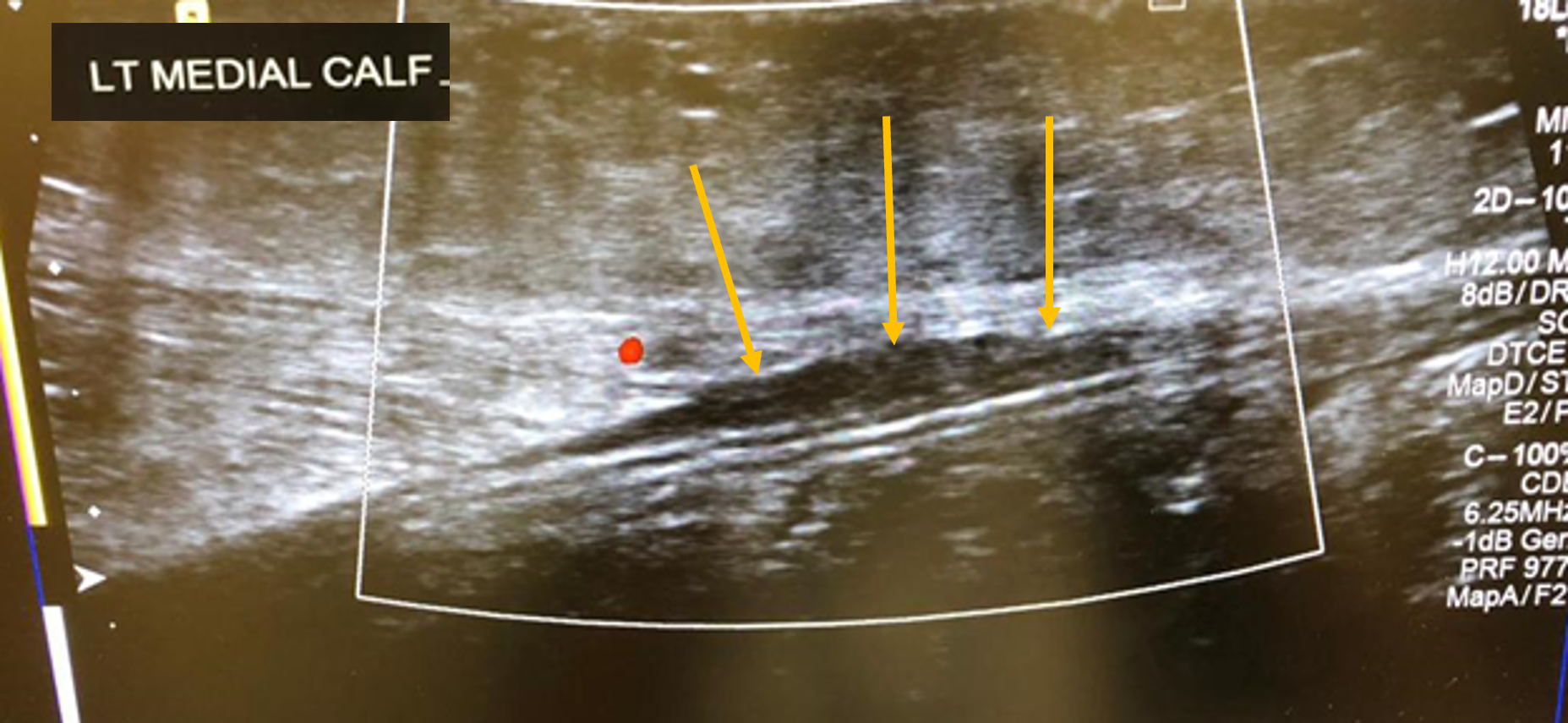
Although classically seen in people who play tennis, it can also be induced by playing squash, skiing, and athletics. Therefore, it typically occurs in active individuals. Extension of the knee and forced dorsiflexion of the ankle seem to be the most frequent biomechanical causes of the injury, which result in rupture of the medial head of the gastrocnemius muscle or injury to the gastrocnemius-soleus aponeurosis, without evidence of muscle rupture.
Ultrasound findings show a hypoechoic linear abnormality (yellow arrows).
To find out more about ultrasound of tennis leg:
Point-of-care Ultrasound Diagnosis of Tennis Leg
Often caused by the force of the tennis racket hitting balls in the backhand position. Forearm muscles, attached to the lateral aspect of the elbow, may become sore from excessive strain.
Tennis elbow, also known as lateral epicondylitis or enthesopathy of the extensor carpi radialis origin, is an enthesopathy (attachment point disease) of the origin of the extensor carpi radialis brevis on the lateral epicondyle. The outer part of the elbow becomes painful and tender. Ultrasound findings include a thickened and hypoechoic common extensor tendon. There is also marked increased power Doppler signal noted, indicating active tendon inflammation. For more information on ultrasound of the elbow and tennis elbow:
1. Musculoskeletal Ultrasound Technical Guidelines II. Elbow
2. Management of Lateral Epicondylitis: A Narrative Literature Review

Tennis players when serving (and plasterers and decorators) are particularly at risk of rotator cuff injuries due to repetitive over arm motions. Ultrasound has great sensitivity for identifying partial tears of the supraspinatus tendon.
The supraspinatus tendon looks like a bird’s beak as it attaches onto the humeral head. A partial tear mimics the eye of the bird. The tear appears as a hypoechoic area within the normal tendon. This mid-substance tear does not extend to the articular or bursal surfaces.
Click here for ESSR Shoulder technical guidelines:
1. Musculoskeletal Ultrasound Technical Guidelines I. Shoulder
and here for:
2. The Application of Musculoskeletal Ultrasound in the Diagnosis of Supraspinatus Injuries
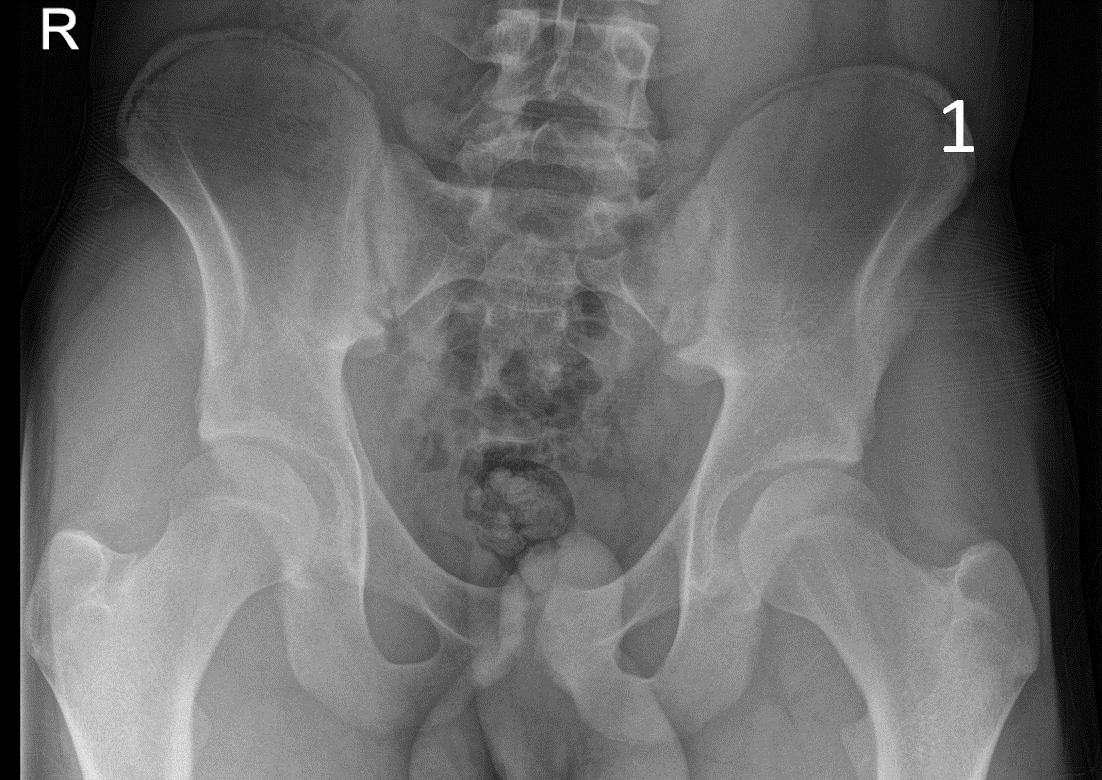
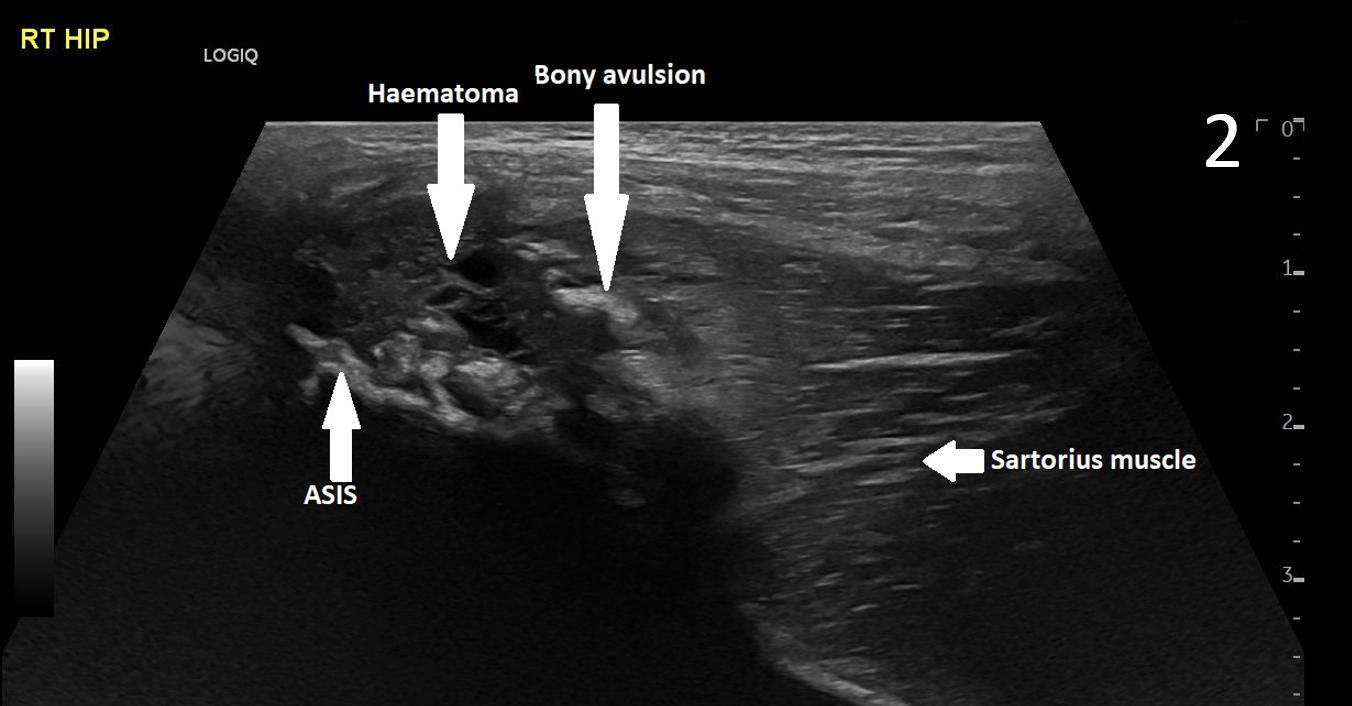
A 17-year-old male presented with severe pain in his right groin. He felt a ‘pop’ in his right groin whilst sprinting and was struggling to weight-bear. A radiograph excluded any bony abnormality (Figure 1) and an ultrasound scan showed no evidence of inguinal or femoral hernia.
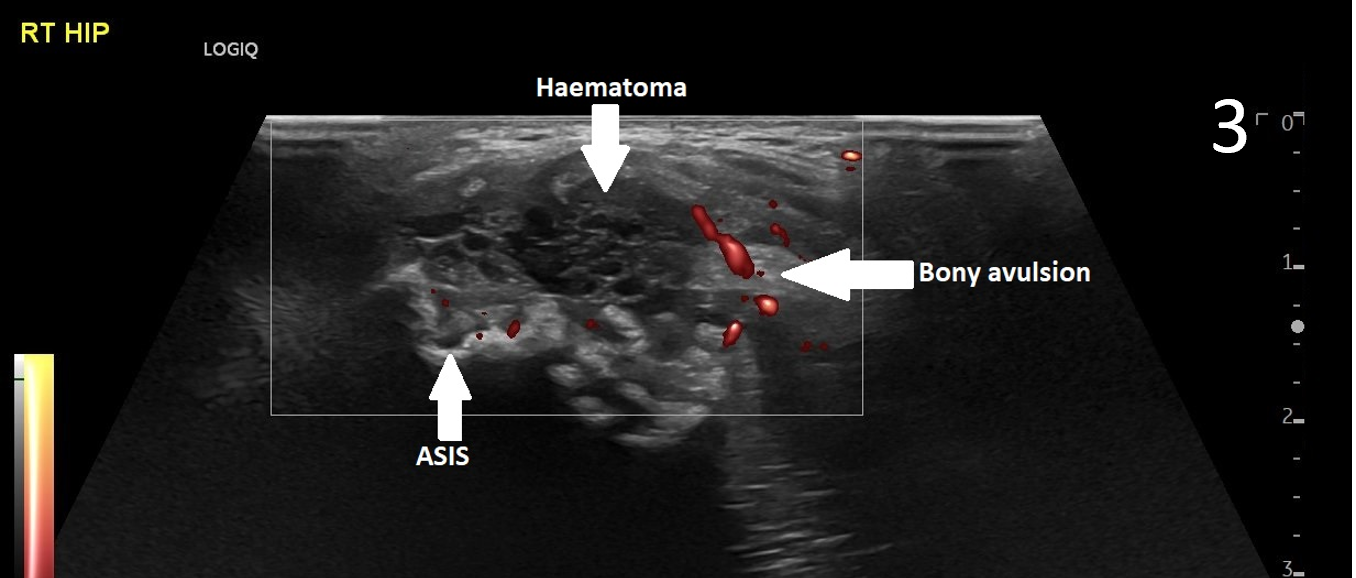
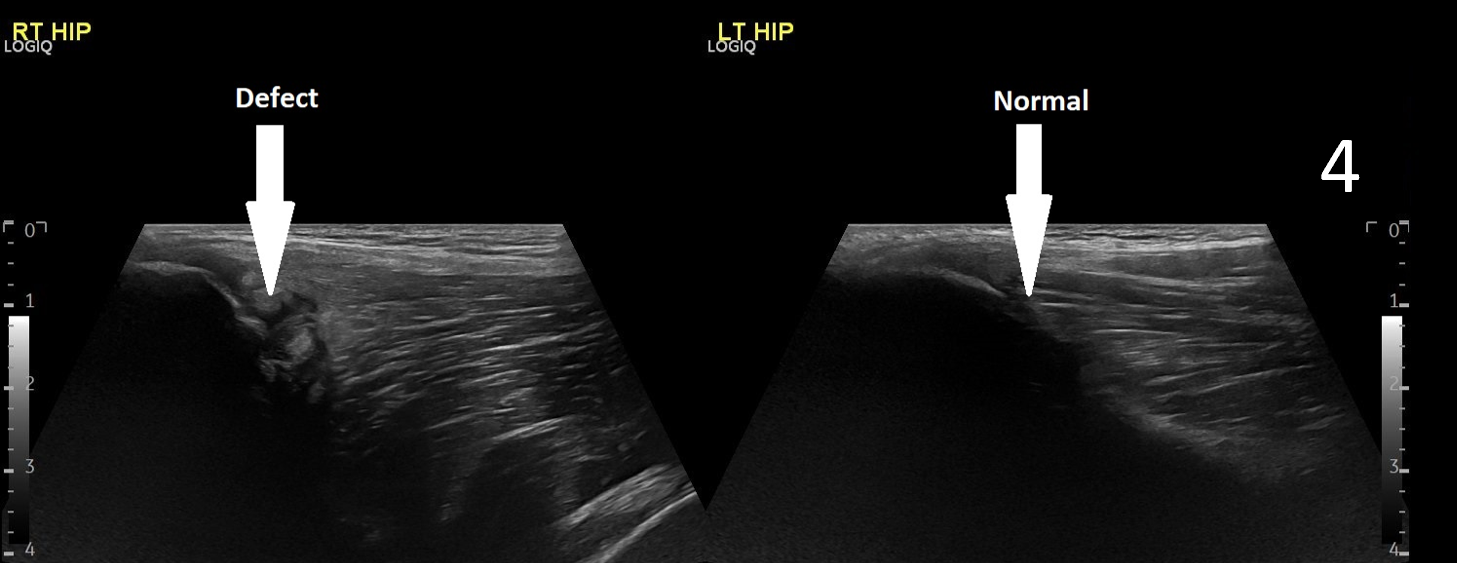
The patient was focally tender in the right iliac fossa at the level of the anterior superior iliac spine (ASIS). At this site, there was muscle fibre disruption and a haematoma at the insertion of the sartorius tendon with minimal retraction (Figure 2). There was cortical irregularity at the ASIS and a bony fragment within the retracted tendon and also neovascularisation here on power Doppler (Figure 3). On comparison to the contralateral side, there was altered architecture of the sartorius muscle with a clear defect while the left side looked normal (Image 4). Ultrasound appearances in keeping with a sartorius tendon avulsion. This was treated conservatively with rest, analgesia and a return to normal activities after two months. Surgical interventions are uncommon and are reserved for when the fracture fragment has migrated more than 3cm.
This injury is associated with young athletes plus young rugby and football players.
Further information:
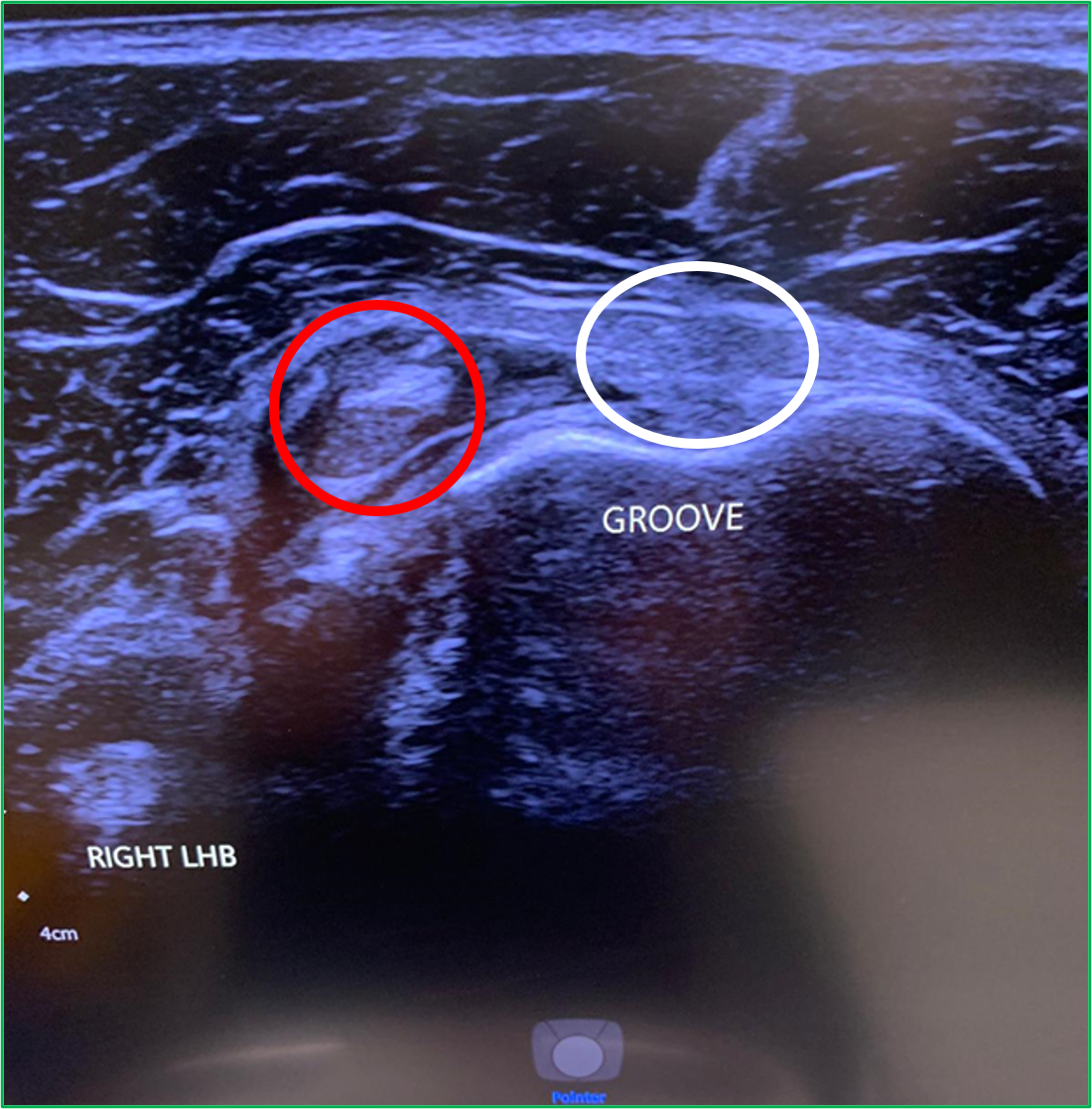
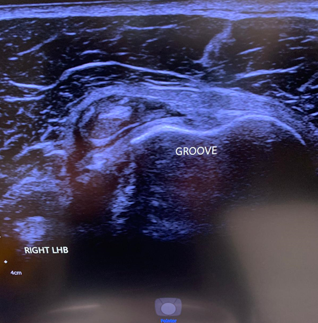
LHB subluxation can happen with contact sports, weight lifting and bodybuilding.
Sometimes the biceps tendon can pop out of its groove. This usually happens because of a tear of the overlying ligament. In other cases, some people are just born with a particularly shallow bicipital groove which puts the tendon at risk of subluxing under load.
Ultrasound findings are of a tendon that is not correctly sited in the bicipital groove (Red circle. The white circle shows where the LHB should sit). To find out more about LHB subluxation:
1. Diagnostic Accuracy of Musculoskeletal Ultrasound on Long Head Biceps Tendon Pathologies
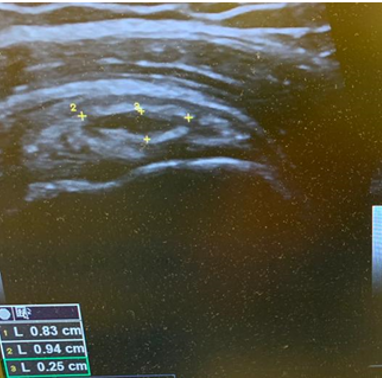
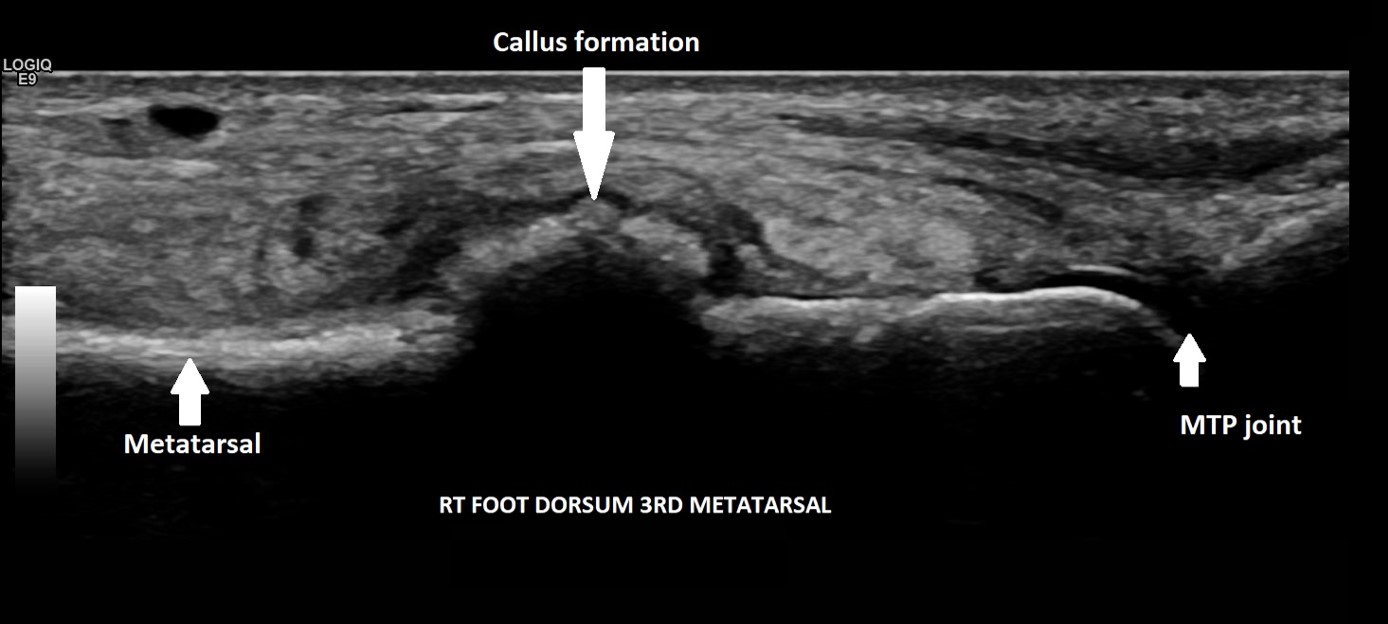
A 29-year-old female, presented with pain and a lump on the dorsum of her right foot. She was training for a 10km run and had been struggling with running over a 6-week period. No history of trauma or erythema to the skin. The clinical suspicion was a ganglion, and the patient was referred for an ultrasound scan for further assessment.
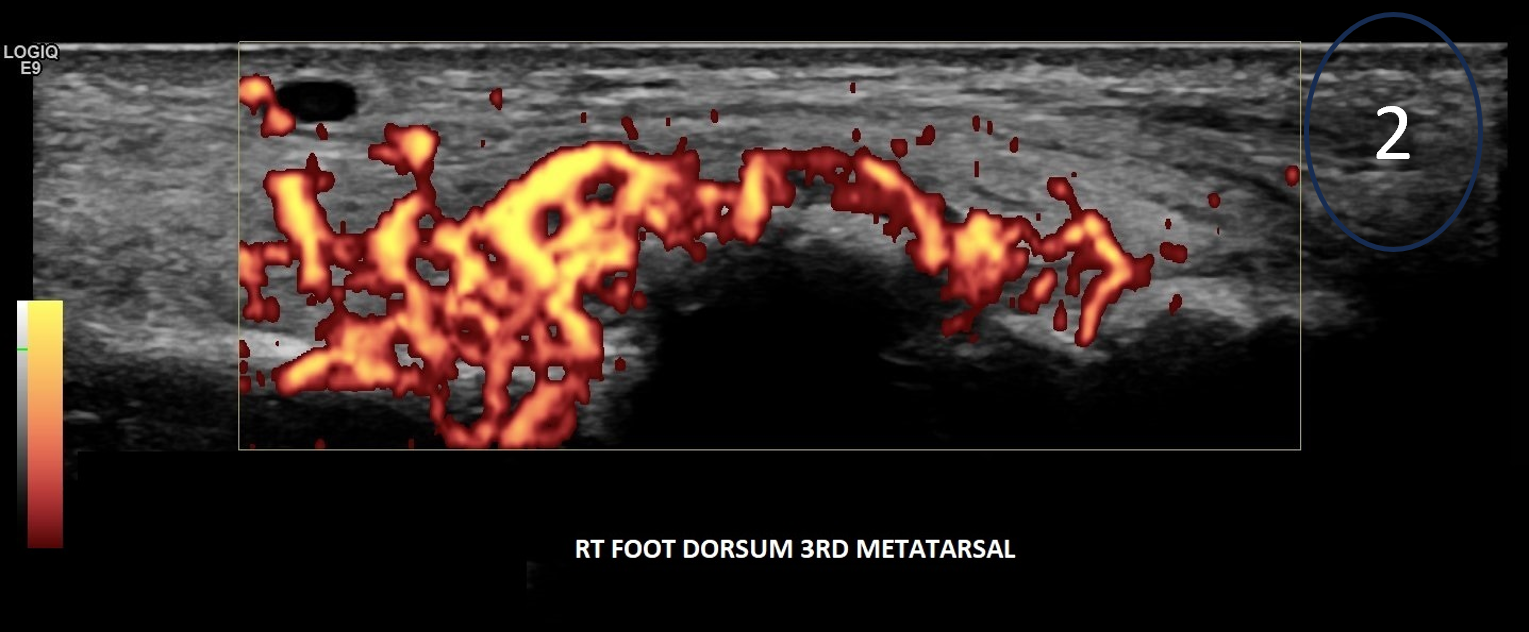
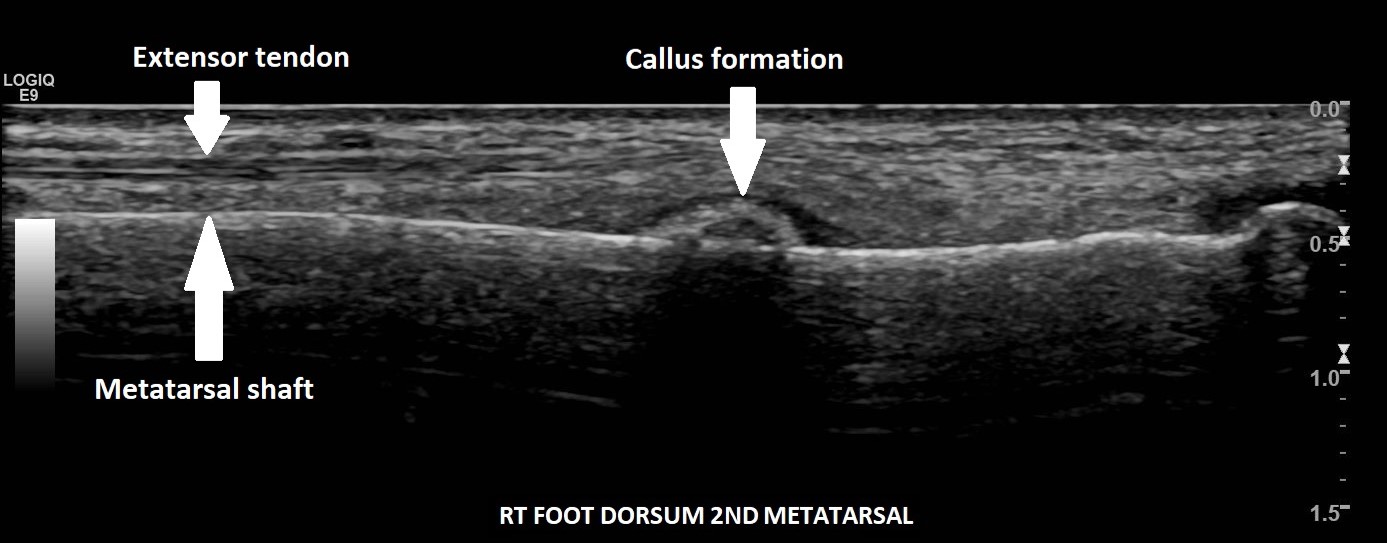
On the dorsum of the foot, ultrasound demonstrated marked cortical irregularity and callus formation around the third metatarsal shaft accounting for the palpable ‘lump’ with surrounding soft tissue swelling (Figure 1). On power Doppler, there was marked peripheral vascularity in the surrounding soft tissues (Figure 2). Incidentally, there was also cortical irregularity and callus formation around the second metatarsal shaft although the patient was not particularly tender here whilst scanning (Figure 3). The cortical irregularity in the second metatarsal shaft was minimal when compared to the third metatarsal and there was no neovascularisation on power Doppler indicating this was an older/mature injury.
Ultrasound appearances in keeping with acute and chronic stress fractures. A radiograph confirmed old and new callus formation (Figure 4). Conservative treatment comprised rest and analgesia. Surgery is generally reserved for stress fractures that do not heal.
Further information see:
1. Ultrasound ability in early diagnosis of metatarsal stress fractures
2. Acute and stress fractures of the metatarsals in athletes

1. Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities